Home | About | Background | Research and Projects | Publications | Team | Contact
Optical Coherence Tomography Angiography (OCTA)
Optical coherence tomography angiography (OCTA) is a new, non-invasive imaging technique that rivals the image quality produced by the current angiographic gold standards, fluorescein angiography (FA) and indocyanine angiography (ICGA). OCTA produces volumetric angiography images in a matter of seconds, by grouping cross sectional B-scans in sets of three, and taking the difference between them to generate a map of blood flow. Thus, varying patterns of blood flow, or regions with a lack of blood flow, are easily distinguished using OCTA. The images produced via OCTA are particularly useful for the evaluation of common ophthalmic pathologies such as age-related macular degeneration (AMD), diabetic retinopathy, and glaucoma.
The acquisition of one OCTA volume takes approximately three seconds, and several volumes are usually acquired for each eye. In a clinical setting, this usually results in an imaging process that takes around 15 minutes. Fluorescein angiography, on the other hand, can take up to 30 minutes for imaging and requires the injection of intravenous dye, which poses some health risks. OCTA, on the other hand, is completely dye-free. However, the main benefit of OCTA over the dye-based imaging modalities is the fact that OCTA produces three-dimensional data, and hence can produce en face images of the individual retinal layers, from the internal limiting membrane to the choroid.
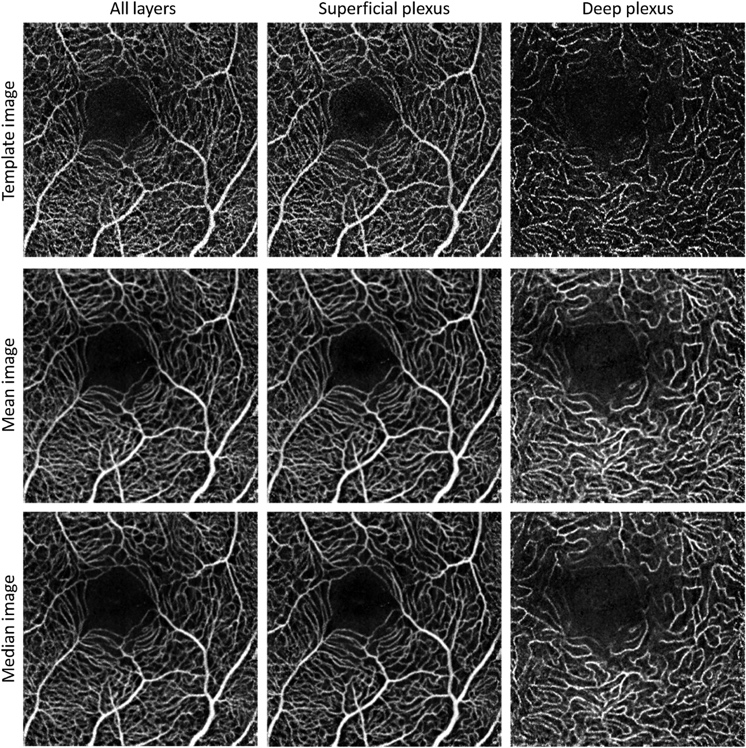
Figure 1: Template image, mean, and median OCTA images (all retinal layers, superficial, and deep plexus) for a healthy male subject, 56 years of age.
M. Heisler, S. Lee, Z. Mammo, Y. Jian, M.J. Ju, A. Merkur, E. Navajas, C. Balaratnasingam, M.F. Beg, M.V. Sarunic, “Strip-based registration of serially acquired optical coherence tomography angiography,” Journal of Biomedical Optics 22(3), (2017)
Adaptive Optics Optical Coherence Tomography (AOOCT) Adaptive Optics (AO) is a technology used to enhance the performance of optical systems by sensing distortions in the measurement medium, and correcting for these distortions by deforming a mirror or by modifying programmable lenses. The technology was initially introduced for astronomy to improve the images acquired from ground-based telescopes by compensating for atmospheric distortions. Recently, however, AO technology has merged with microscopy techniques, resulting in the advancement of biological imaging.
The distortions of the medium can be detected by a wavefront sensor, or by using the image quality as a metric to deduce the optimal shape of the deformable mirror. When combined with OCT, AO can greatly improve the resolution of the cell layers, including the photoreceptor mosaic, allowing for clear visualization and segmentation of individual photoreceptors and nerve fibre bundles. In practice, however, the enhanced resolution provided by this technology comes at the price of a large and complex system when a wavefront sensor is used. Hence, this is the main motivation for the development of wavefront sensorless adaptive optics (WSAO), as it aims to gain the enhanced resolution of the AO technology without the added hardware complexity.
Y. Jian, S. Lee, M.J. Ju, M. Heisler, W. Ding, R.J. Zawadzki, S. Bonora, M.V. Sarunic, “Lens-based wavefront sensorless adaptive optics swept source OCT,” Scientific Reports 6, (2016): 27620.
| Before Optimization | After WSAO Optimization |
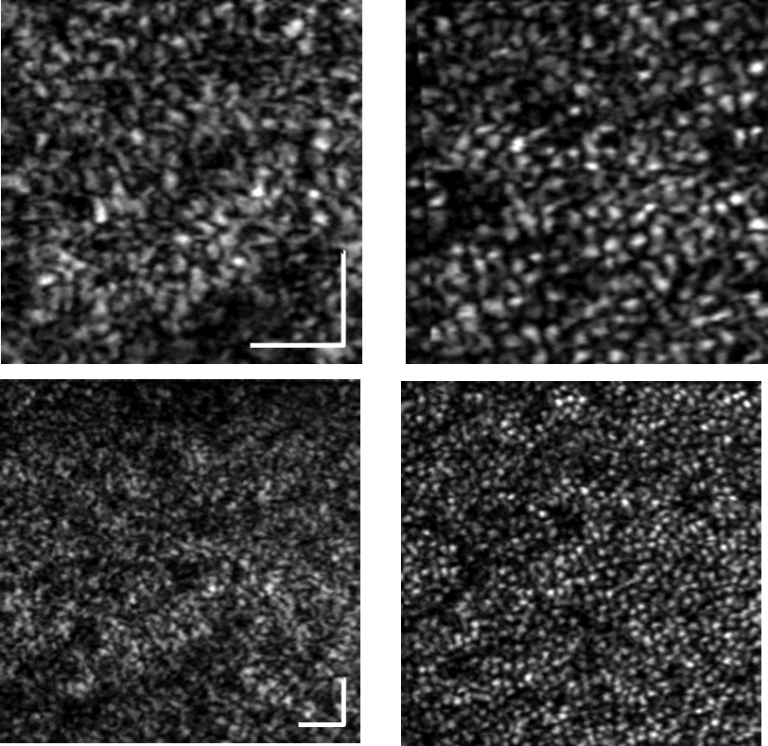
Figure 3: Human retinal imaging with: |
|